When Clinicians ‘Find the Fault’ Their Trained Brains Might Work Against Them...
Ever had a moment where someone points out one tiny crack in a beautiful vase, and suddenly all you see is that crack? Clinically speaking, it's like dismissing an otherwise excellent lab proposal because of a minor formatting error, while the real magic of the project gets lost in the noise.

Ever had a moment where someone points out one tiny crack in a beautiful vase, and suddenly all you see is that crack? Clinically speaking, it's like dismissing an otherwise excellent lab proposal because of a minor formatting error, while the real magic of the project gets lost in the noise.
In clinical trials, our training often trains us to find the fault. After all, under-scrutinising could risk patient safety. Problem is, that needle-focus can tip into over-perfectionism. Instead of judging things mostly good, sometimes we dismiss them because they’re not flawless.
In this article, I unmask that tendency, unpack how it can backfire, and challenge us to shift from a micrometer mindset to a “whole-process” perspective. Let’s treat near-perfect proposals and ideas with the respect they deserve, even if they carry a tiny blemish.
Example: The Proposal That Got Nixed
Picture this: an investigator submits a brilliant protocol: on-time recruitment, a participant-centric ePRO strategy, and a statistically sound design. But the formatting is off, the tables misaligned, and a typo in the title. The reader, trained to see flaws, flags it. The proposal gets shelved, not because of content, but cosmetic issues.
That tiny “find the fault” impulse short-circuited good science.
Real-World Backfire: Confirmation Bias in Transplant Diagnostics
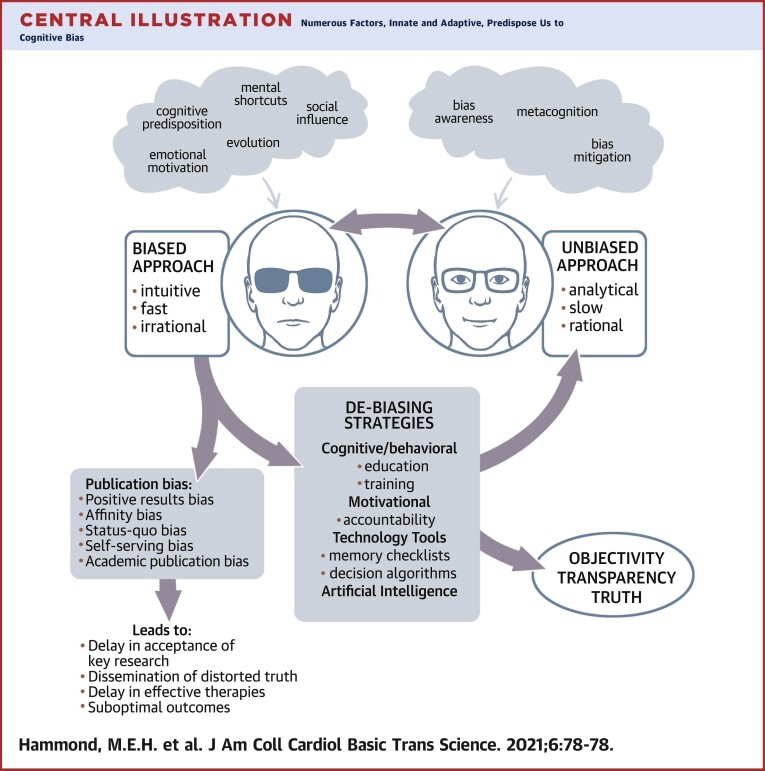
In a classic clinical case, researchers originally underestimated the role of certain antibodies in transplant rejection because they sought evidence that confirmed existing beliefs. Confirmation bias delayed scientific progress and continued rejection-related deaths. Only when the bias was acknowledged and debiased did researchers start accepting the actual immunological signals pointing to true causes. This illustrates how fault-finding, when it leans into bias, can derail outcomes that matter deeply. (Hammond, 2021)
Why This Happens
Perfectionism and Cognitive Bias: Our training rewards us for spotting flaws, but unchecked, that becomes clinical perfectionism, where even small deviations overshadow the bigger picture. (Shafran, 2002)
Einstellung Effect: Past experience trains us to apply familiar problem-solving patterns, even when new, better solutions exist. In the lab, that means rejecting protocols for reasons we’ve rejected before, even if they deserve a fresh lens. (Wikipedia, 2025)
Confirmation Bias: Once we have an expectation, we see confirming evidence—and dismiss contradictory signals. It’s why some diagnostic breakthroughs get delayed, not because they’re wrong, but because they don’t fit our mental model. (Parmley, 2006)
What to Do Instead
Start with “mostly good.” Ask: What does this do well? Then, what are the minor tweaks needed?
Debias the review. Include a quick checklist: “Does this fundamentally work?” If yes, escalate instead of reject.
Think process first. Focus on whether the workflow or methodology is sound, not on the formatting, labelling, or minor missteps.
Cultivate detective curiosity. Are we rejecting it, or maybe misunderstanding it? Asking “What could go right?” opens thought, not shutting it down.
Conclusion
Sometimes, training to find the fault actually blocks the very breakthroughs we seek. Whether it’s dismissing a winning proposal over cosmetic errors or delaying life-saving diagnostics because of confirmation bias—we lose when we fixate on perfection instead of potential.
Let’s retrain our minds to start with “mostly good,” not “mostly flawed.”
References
Hammond, M.E.H. (2021). Bias in Medicine: Lessons Learned and Mitigation Strategies. PMC.
Shafran, R. (2002). Clinical perfectionism: a cognitive–behavioural analysis. Behaviour Research and Therapy.
Luchins, A.S., & Luchins, E.H. (1959). Einstellung Effect. Wikipedia.
Parmley, M.C. (2006). The Effects of the Confirmation Bias on Diagnostic Decision Making. Drexel University Dissertation.
No clinicians were offended in the researching and writing of this article.
About

Delivering independent journalism, thought-provoking insights, and trustworthy reporting to keep you informed, inspired, and engaged with the world every day.
Featured Posts








